Why We’re Fighting for the Same Drugs Our Neighbors Have in Canada
- Stacy

- May 14
- 6 min read
My daughter is 15 years old.
She keeps rescue medication in her backpack. One dose. Donated to us, because without that generosity, she would have none at all. If she uses it, there is no more. There is no prescription waiting at the pharmacy. There is no refill covered by insurance. There is just the hope that she doesn’t need it again before we figure out how to replace it.

She has learned her triggers. She knows that stress, a bad sleep, or pushing herself too hard can be the thing that starts an attack. She knows that if her throat starts to tighten, she needs to act fast. She knows all of this because she has to.
There is a medication that could save my daughter during her most dangerous moments. It is approved in Canada. She cannot have it. Not because it doesn’t exist. Not because it doesn’t work. Not because her doctor hasn’t tried to get it for her. Not because we haven’t fought. But because the type of HAE she has doesn’t meet the criteria for coverage. Because of a bureaucratic technicality in a system that was never built with her in mind.
She should not have to ration her only dose of life-saving medication and hope for the best. She should not have to know her triggers at 15, the way most teenagers know their Spotify playlists. She should not have to be this brave. But she is, and until the system changes, I am going to keep talking about it. Loudly.
What Is HAE?
HAE stands for Hereditary Angioedema. It is a rare, genetic condition that causes sudden, painful, and potentially fatal swelling of the face, throat, stomach, hands, feet, genitals and other body parts. It affects approximately 1 in 50,000 people. It is hereditary, with a 50/50 chance of being passed to your children.
The drug that works, that can save us, is called icatibant, and in Canada, for patients like my daughter and me, it is still out of reach.
Our Story

My family and I have both been living inside this disease for nearly ten years. We know what it feels like to have your body turn against you without warning, to keep a packed hospital bag by the front door, to explain your swollen face to people who look at you with blank stares and say nothing useful. But our experiences are not identical, and that difference is exactly the problem I am writing about today.
I have HAE with normal C1-inhibitor (HAE-nC1INH), formerly known as Type 3. It's the type that doesn't show up on standard bloodwork, the type that took years to diagnose, and the type that carries the most barriers to treatment access in this country. My sister Amanda has HAE Type 1. The type with measurable C1-inhibitor deficiency. The type that shows up on bloodwork. The type that qualifies for treatment.
Here is the best way I can explain what that difference means in real life:
Imagine you have a severe food allergy. You go to your doctor, you test positive on the scratch test, and you are immediately prescribed an EpiPen. Covered. No fight. No waiting. Your life is protected.
Now imagine your child has the same reaction to the same food. The same symptoms. The same fear. The same full-body hives. But their scratch test comes back negative. So, they don’t qualify and are sent home without the EpiPen.
That is what it is like to have HAE with normal C1INH in Canada rather than Type 1 or 2.
Same disease. Same danger. Different access.
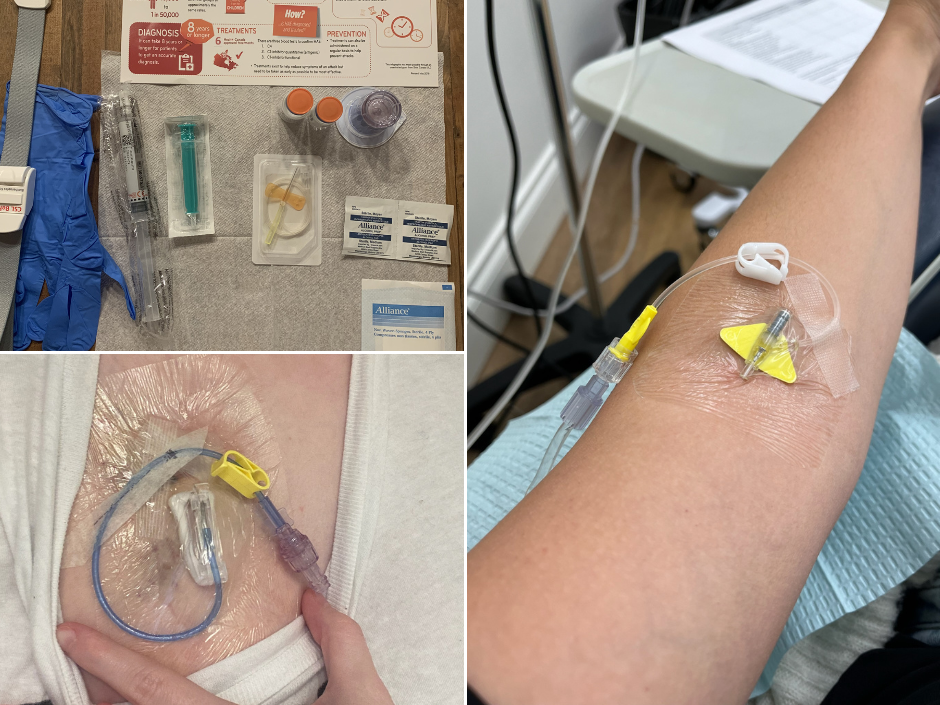
I spent years on IV treatments I gave myself at home, over 500 of them. I blew every vein I had. I had a chest port surgically placed just to be able to administer the medication keeping me alive. I eventually gained access to a preventative medication, but only through a clinical trial. It is still not approved in Canada for patients with HAE with normal C1INH. I had to fight my way into a trial just to access something that works.
My daughter is 15. She has the same type of HAE as me. She is managing a life-threatening disease with fewer tools than she deserves, because of a bureaucratic technicality that means her paperwork doesn't check the right boxes. And she is not alone in this fight.
The Drug That Should Be Everywhere And Isn't
Icatibant is a rescue medication for HAE attacks. It is a subcutaneous injection, a needle under the skin, that targets the bradykinin receptor responsible for causing the swelling. It works quickly. It is self-injectable and designed to be used at the first sign of an attack, before things become catastrophic.
Think about how we treat severe allergic reactions in this country. We don't make people wait to get to a hospital before accessing epinephrine. Kids carry EpiPens in schools. We carry them on planes. We train people how to use them. We make them available because we understand that in an anaphylactic emergency, minutes matter. HAE attacks are no different.
A throat attack can close someone's airway in minutes. An abdominal attack can be so severe that it mimics appendicitis and results in unnecessary surgery. And unlike anaphylaxis, HAE does not respond to the tools first responders actually carry.
Patients are transported to hospitals that may not have the medication to stop the attack. Families who carry their own supply have learned to bring it with them to the ED and administer it themselves, or watch staff fumble through a protocol they have never encountered before.
This is the standard of emergency care for a potentially fatal condition in Canada in 2026.

In December 2024, Canada's Drug Agency released its Implementation Advice for icatibant, stating it should be available to all HAE patients, including those with HAE with normal C1INH, people like my daughter, my sister, my mom, my nieces and me. The recommendation is there, in writing, from the national drug agency.
But provincial formularies haven't moved.
The guidance exists. The drug exists. The need is urgent and documented, and yet all patients with normal C1INH are still waiting.
We Stopped Waiting
For years, I showed up to HAE Awareness Day and shared my story, hoping that visibility alone would create change. And visibility matters. I still believe that. But at some point, sharing stops being enough.
This past year, Amanda and I both joined HAE Canada, a national patient advocacy organization, as volunteers on its Advocacy Committee. On our own time. Because we are done sitting on the sidelines while my family and hundreds of others like us wait for a system to catch up to their reality.
We are at the table now.
We are part of the conversations happening with provincial governments, with healthcare decision makers, with the people who control whether icatibant makes it onto a formulary for normal C1INH patients like us. We are bringing my family's story, nearly ten years of it, into rooms where policy gets made.
And it is the most important thing we have ever done outside of raising our kids.
We are not doing this because we have spare time. We are doing this because my daughter is 15 and still managing a life-threatening disease without the full toolkit she deserves. Because there are people in this country who have never heard of HAE, who are sitting in emergency rooms right now being given medications that won't help, who deserve better than what the system is currently offering.
What You Can Do Right Now
HAE Canada is currently running a letter-writing campaign calling on provincial governments to add icatibant to their drug formularies for all HAE patients, including those with HAE with normal C1INH.
And this fight is not just for patients like us.
Even Canadians with HAE Type 1 and Type 2, the types that show up on bloodwork, the types that qualify for more, are not fully protected. Many are facing unaffordable deductibles and copays that make treatment out of reach financially. Some still cannot access icatibant in their province. The access crisis in this country touches every type of HAE patient in one way or another.
Canada's Drug Agency has already recommended that icatibant be available to all HAE patients. All types. No exceptions. Now the provinces need to act.
Send the letter. Share this post. Tag your MLA or MPP. Put it in your stories. Send it to your doctor, your pharmacist, your neighbour who works in health policy.
The last campaign generated over 220 letters. They are calling for more. This round matters.
We Are Louder Than Ever
Last year, we asked you to see us. This year, we are asking you to stand with us. Not just by reading and sharing, though please do both, but by understanding that awareness without action is just noise.
The system will not change on its own. It changes because patients, families and communities refuse to accept that a 15-year-old girl with a potentially fatal disease deserves less access to emergency medication than someone with a different diagnostic code.
We are at the table. We are making noise. We are not going anywhere.


I am also recently diagnosed with HAE c1N INH. I have a prescription for Icatibant but it is $1600 per dose. Beyond my pay grade! I checked both my local hospitals and one carries it. I also have a letter I carry from my immunologist outlining my care. But it’s just so ridiculous for me to have to go to ER when it could be prevented. I’ve also been in contact with my MLA and BC Pharmacare. I will definitely be wearing purple on May 16th